Both founders and researchers in healthcare are spending far too much of their energy in areas where they’re not going to make maximum impact. Most health problems are self-inflicted, but the innovation economy doesn’t reflect the power of preventive healthcare. Dr. An Nguyen and I just completed an analysis of VC and research funding compared with the cost to society of different diseases, and the results show wildly disproportionate funding for certain diseases relative to their impact in society. It also shows market white space for the smart entrepreneur.
The data is painful. Obesity alone was responsible for 9.1% of US annual medical costs in 2008, compared with 6.5% a decade prior. Eight simple risks and behavioral choices drive 80% of total costs for all chronic illnesses worldwide, and 86% of US health care spending is on treatment of those chronic diseases. According to the WHO, if the major risk factors for chronic disease were eliminated, at least 80% of all heart disease, stroke, and type 2 diabetes would be prevented, and over 40% of cancer cases would be prevented.
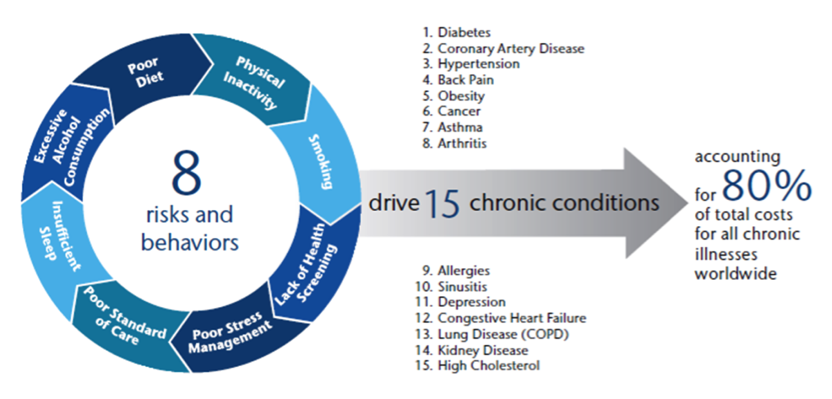
Source: AON Hewitt 2012 Health Care Survey, based on World Economic Forum data.
The good news is that we already have effective medical solutions to most medical problems the average person has, both the self-inflicted (listed above) and others (most wounds, many diseases, etc.) Even for such scary diseases as cancer, we have far better treatments than was true historically. If you just take reasonable care of yourself and avoid any major accidents, you can live at least 78.7 years, the average US life expectancy.
Yet, the bad news: US life expectancy ranks #26 in the world, well below many less wealthy nations which spend far less on healthcare than we do. There are multiple reasons for that, but a major one is that both VC and research funding is concentrated in areas where there appears to be short-term revenues, as opposed to areas that will save more lives and quite likely generate both long-term revenues and savings for society. According to the CDC’s funding data, just $32 billion of 2010-2014 spending was related to “prevention”, vs. a total of $168 billion for all disease categories combined.
The healthcare research system is spending lots of time and money on the edge cases, e.g., studying rare diseases, or refining their predictive models for exactly how much more likely you are to have a certain cancer if you have two children vs. zero. At the same time as researchers complain about lack of research budget, the scarce dollars allocated do not appear to be aligned with the areas where the greatest impact can be achieved.
The industry standard metric for tracking the severity of disease is disability-adjusted life years (DALYs), i.e., the number of healthy life years lost due to the disease or risk. Although cardiovascular disease exacts the highest costs in DALYs of any disease, the $13B in total VC and NIH funding for cardiovascular diseases only represents 38% of cancer funding and 57% of infectious disease funding.

All venture capital and NIH funding data for CY 2010 – 2014 in USA. Source: NIH, CB Insights. Ideally, we’d include other healthcare funding sources (corporate R&D, university, and private foundations), but haven’t found a comprehensive source for this information.
Disability-adjusted life year (DALY) for CY 2010 in USA, multiplied by five. Source: WHO, IHME.
NB: Annual cost in DALYs (millions) is 2.56 for diabetes and 2.69 for infectious diseases. Bars for diabetes and infectious diseases are displayed slightly offset to aid comparison.
NB: HIV/AIDS represents 68% of funding for infectious diseases, which means that many diseases more infectious and likely far more dangerous than HIV/AIDS but with weaker lobbies (e.g., Ebola and SARS) are receiving disproportionately low funding.
A standardized way to look at the issue is to calculate funding per DALY, i.e., the amount of venture capital (both private and corporate) and NIH research funding allocated to combat each year of healthy life lost. Cardiovascular diseases have received only 34% of cancer funding per DALY, 32% of diabetes funding per DALY, and 18% of infectious disease funding per DALY. Even more striking, cardiovascular diseases, obesity, tobacco use, and alcohol use combined receive less funding per DALY than diabetes or cancer alone.
We found disproportionate funding occurring not only across diseases and risks, but also in the allocation towards prevention. When we look at NIH funding of cancer, cardiovascular, diabetes, infectious disease, and alcohol use, 25% to 39% of the funding is in prevention-related research. By contrast, 60% of tobacco and 94% of obesity NIH funding is related to prevention.
An experienced healthcare researcher friend observed that for the preventable/lifestyle diseases that comprise the vast majority of US healthcare spending, “I think there would be substantial benefit toward encouraging higher-quality research on prevention and reduction of healthcare costs, e.g., focus for heart disease should not be “just” finding a new drug, but also preventing high blood pressure by motivating people to eat less salt AND continue to do so for the rest of their lives. What little funding there is for such research is generally short-term (roughly a 6-month intervention) or represents minor modifications of past research (e.g., study #1: show patients a video on the benefits of weight loss; study #2: show patients a video + call them once a week for 6 weeks to motivate them more). This is not big picture. I think that research needs an overhaul to think about non-traditional ways of reducing disease.”
Dr. Nguyen observes that the NIH is taking note of some issues with misallocation of funding incentives. One of their arms is going to pilot a new approach next year. At the American Society for Cell Biology Conference last month in Philadelphia, they described their approach as emulating venture capital by maximizing investigator productivity and investing in a portfolio of strong investigators.
According to the CDC’s must-read report on The Power of Prevention, the low-hanging fruit to improve our national health (and therefore I suggest create new businesses) includes:
– Health promotion to encourage healthy living: make better food choices, quit smoking/heavy drinking, and live a more active lifestyle. This also includes changing economic incentives, e.g., Mayor Bloomberg’s successful “nudges” to raise taxes on cigarettes and make it much more difficult to smoke indoors.
– Early detection, such as screening at-risk populations. Blood pressure screenings at churches are an often-used example of effective community-based partnerships.
– Improve training and education of health care professionals to connect patients with existing resources and tools, particularly early diagnosis and screening; most doctors are using decades-old technology.
– Improve logistics to get the basics of competent treatment to people more quickly, e.g., improve the level of sanitation in lower income regions; provide universal fluoridation and vaccination.
(The CDC doesn’t discuss it, but I would add that one of the best ways to promote health is to spend the relatively small amount of money required to prepare for predictable, high-impact adverse events, e.g., pandemics, solar flares/electromagnetic pulse attack, and catastrophic weather. See the Lifeboat Foundation and The Gray Rhino: Why We Keep Missing the Most Obvious Threats -And How We Can Get Out of Their Way for more on this topic. Unfortunately these problems are not well suited to a private sector solution, but preparing for disaster is a classic public good which competent governments should be preparing for.)
So shouldn’t the entrepreneurial energy in healthcare, and more of our collective charitable/tax dollars, be focused in the high-impact areas?
I think I understand why a lot of entrepreneurs in healthcare are pursuing the areas that also attract research dollars: there are lots of revenues associated with new drugs and treatments. Under our current absurd healthcare system, there’s more money to be made treating diseases, than stopping them from occurring. Healthcare founders are being rational in an irrational system.
I suspect this allocation of energy is driven by both perverse incentives and momentum. Diseases with strong lobbies (e.g., breast cancer, AIDS) get disproportionate funding. More broadly, most healthcare researchers are trained in medicine and statistics. They’re not usually trained in psychology, marketing, business, or economics. The peer review processes for research grants exacerbate this by focusing criteria for a research project on impact within that specific field, missing an opportunity to assess the potential impact with societal outcome measures such as DALYs. When impact on society is considered, it is lumped into a laundry list of broader criteria and considered optional. So researchers tend to approach their work through a lens which may not highlight the most relevant factors, the fact that psychological and economic levers are pushing people towards self-defeating behaviors. Also, the elites who fund a lot of medical research have fewer self-caused medical problems such as obesity and tobacco addiction, so I suspect they have a motivation to focus their charitable support on less common diseases which might impact them personally, e.g., genetic diseases and HIV/AIDS.
The Copenhagen Consensus has done some innovative work helping funders think rationally about the prioritization of their spending, and I think the Bill & Melinda Gates Foundation and Robert Wood Johnson Foundation have also been thoughtful about allocating research dollars in a more rational way. Dr. Atul Gawande has a fascinating article on the BetterBirth Project, a rare successful effort to promote behavior change, in this case in reducing infant mortality in India. As he observes, behavior change (such as prevention) is possible, it’s just expensive. With those and some other honorable exceptions aside, it appears that a significant misallocation of money and energy is directly hurting our national health level.
Our firm does virtually no investing in life sciences, and historically has also been adverse to healthcare IT startups, given the long sales cycles, heavy regulatory burden, and our own lack of internal knowledge in these sectors. However, we’re interested in companies which can serve millions of people and also have a low regulatory burden. The health-related companies in which we invest reflect those biases, and we think have potential to help very large groups of people at low marginal cost. Thousands of people are using Interaxon’s brain-sensing headset to address depression, stress, ADHD, PTSD, etc. Folks are using Plated’s fresh meal kits to improve the quality of their nutrition. Parents are using Owlet (currently in beta) to monitor the health of newborns. Parents are also using Volunteerspot for, among many other purposes, organizing campaigns at their schools to promote healthy food. Authorea addresses inefficiencies in the very early stages of the research lifecycle, making the writing of research more efficient, more collaborative, and more transparent. In turn, with more open, transparent, and data-driven scientific publishing, healthcare research can move faster and be subject to a higher level of review and scrutiny.
I don’t know how to solve this problem, other than that when I meet young researchers/founders in healthcare, I encourage them to study economics and marketing as well as traditional medicine as a vector to promote health. Our medical problems are too severe for doctors alone to solve.
Thanks to Dr. An Nguyen, founding and former managing partner at Dorm Room Fund, for original analysis, and Rick Lipkin, Venture Partner at Easton Capital Investment Group. Thanks also to an anonymous friend in the healthcare research industry for thoughtful review of this article. The fact that he chose to be anonymous may say something about how sensitive this issue is. Previously posted in PEHub.